Liver Transplantation for Hepatocellular Carcinoma
THE METROTICKET PROJECT
WELCOME! You have just entered the Metroticket website: a project originally endorsed by ELITA (European Liver and Intestine Transplant Association) and ILTS (International Liver Transplantation Society) in order to give evidence to the clinical management of patients with hepatocellular carcinoma (HCC) undergoing liver transplantation.
The original idea, developed on the tumor explant pathology of more than 1000 real life transplants for HCC beyond Milan criteria, produced not just the up-to-7 criteria (Lancet Oncology 2009) but also a user-friendly calculator to predict the post-transplant survival of a given patient, according to the maximum size of the tumor, number of tumor nodules and presence/absence of microvascular invasion.
In this restyled version, besides the original calculator, you may find the additional option of a prognostic calculator based on pre-transplant tumor determinants at radiology staging (e.g. maximum size of the vital HCC and number of vital HCC nodules) combined with the serum alpha-fetoprotein (AFP) level. The additional calculator is aimed at capturing morphology and biology of the tumor at presentation as well as before and after application of neoadjuvant or downstaging treatments. In addition, the overall prediction of survival (with confidence intervals) can be selected according to presence or absence of history of HCV infection.
INSTRUCTIONS
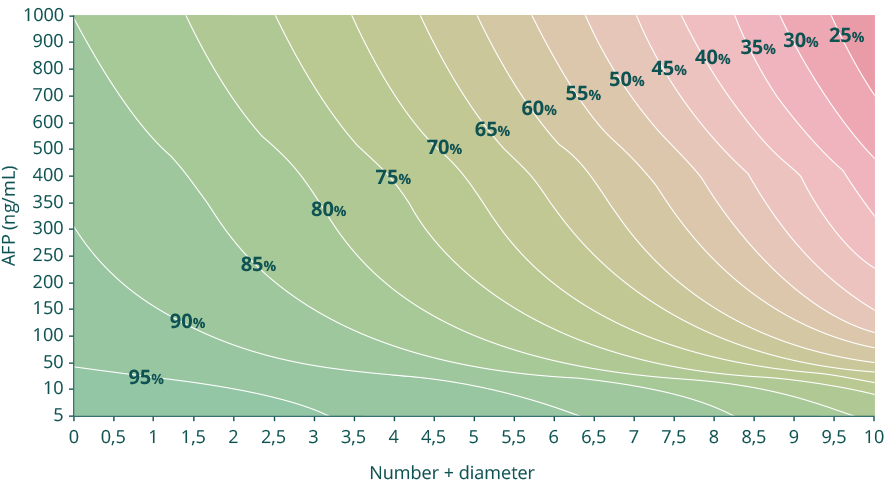
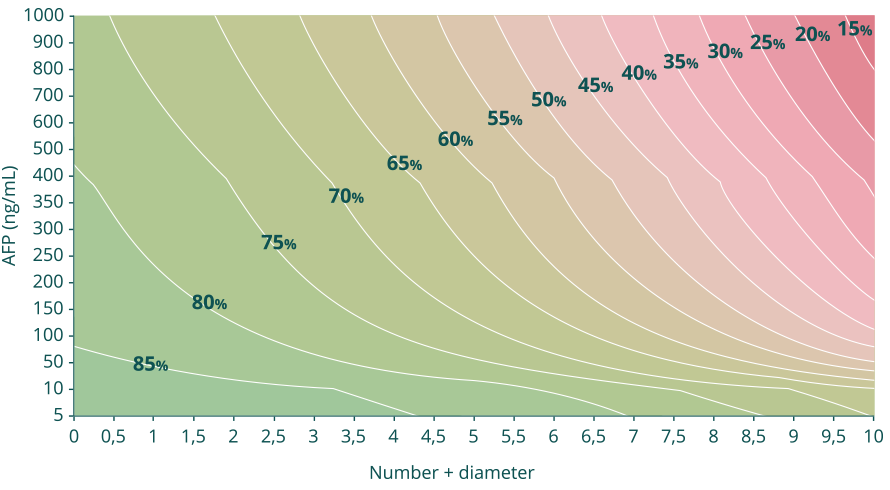
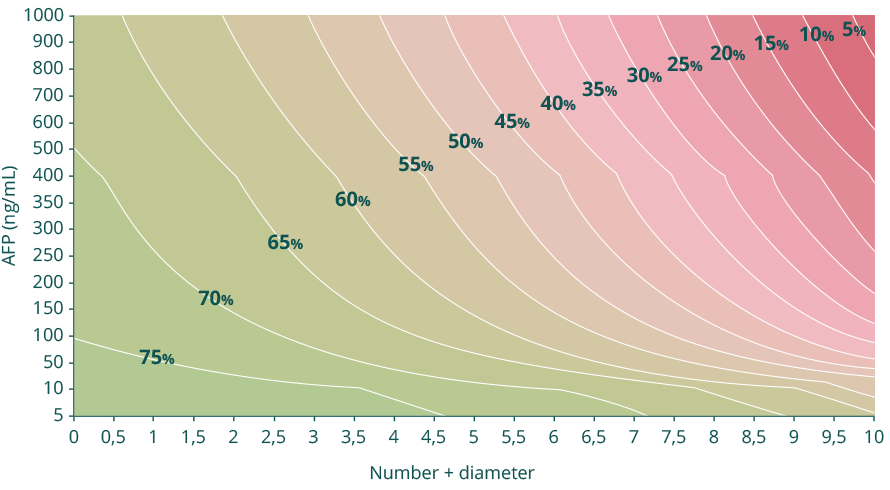
1. Scrolling down on the website, the Calculator named “Post-transplant survival according to HCC pre-transplant staging and AFP” gives you a 5-year post-transplantation prediction of HCC specific survival based on the pre-operative radiological tumor assessment.
Select size of the largest (vital) tumor and the number of (vital, ≥1cm) tumor nodules and add the last AFP level (in ng/mL). The “calculate” button will then generate the prognosis.
The overall prediction can be refined by choosing presence or absence of HCV cirrhosis in the transplant candidate, in order to calculate overallsurvival without the interference of the co-morbidities caused by the persistence of HCV infection after transplantation.
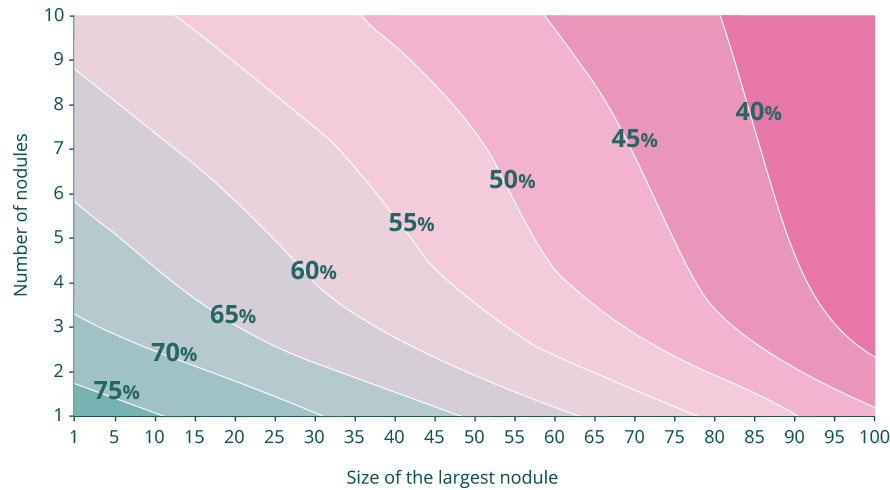
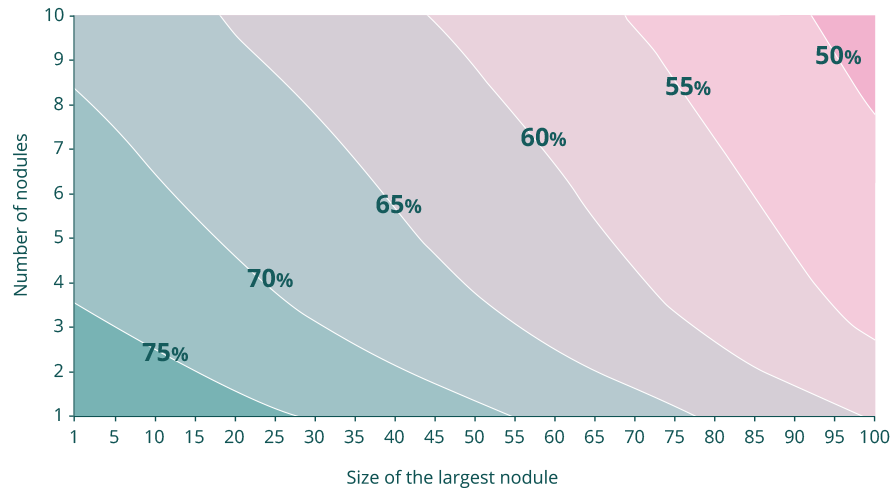
2. The second Calculator named “Post-transplant survival according to HCC pathology” is the original Metroticket calculator (Lancet Oncology 2009), built to generate a five year overall survival prognostication on the basis of histological features at explant pathology; choose number of nodules and add size of the largest of these to have a 5 yr estimation of survival. This result can be then refined by choosing presence or absence of microvascular invasion.
The prediction of survival can be saved in your electronic storage in order to be shared, viewed, and printed.
Pre-operative radiology + alpha-fetoprotein
Size of the largest vital tumor
0 cm
Number of vital nodules
0
AFP (ng/mL)
5
5-year predicted HCC-specific survival after liver transplantation: %
95% confidence interval: - %
5-year predicted survival after liver transplantation: %
95% confidence interval: - %
5-year predicted survival after liver transplantation: %
95% confidence interval: - %
Post-operative pathology*
Size of the largest nodule
0.1 cm
Number of nodules
1
5-year predicted survival after liver transplantation: %
95% confidence interval: - %
5-year predicted survival after liver transplantation: %
95% confidence interval: - %
5-year predicted survival after liver transplantation: %
95% confidence interval: - %
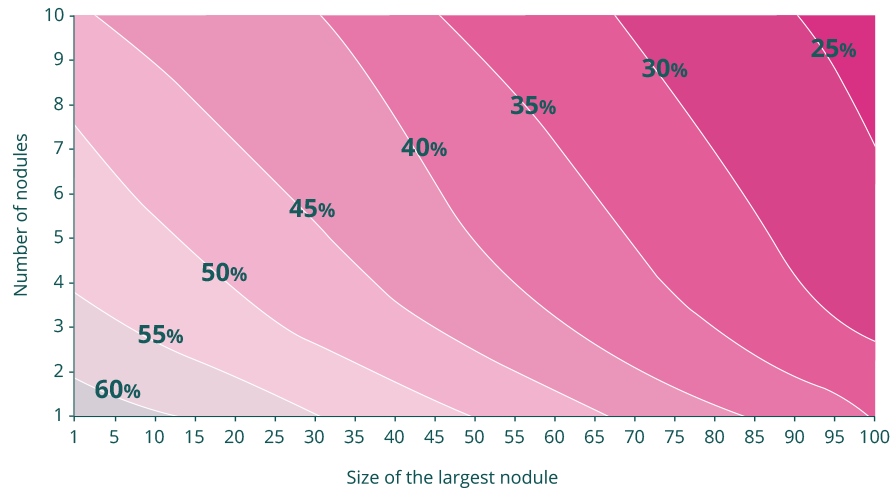
* Mazzaferro V, Llovet JM, Miceli R et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet Oncol. 2009;10(1):35-43.
We hope that, in the perspective offered by liver transplantation for HCC, the individualized prognosis delivered by the calculators will help sharing decision-making between clinicians, patients and regulators.
The Metroticket Project Team
The derived prediction of survival can be saved in your electronic storage
in order to be shared, viewed, and printed.